

Orthodontic Treatments

Treatment lengths
Orthodontic treatment lengths vary by individual. Some minor treatments can be accomplished in a few months while the treatment of more severe malocclusion can require two or more years. We do know for sure that patients can and do influence the treatment time and outcome. Excellent cooperation including good oral hygiene and home care, avoidance of damaging hard and sticky foods and candy, regular wear of removable appliances when indicated and keeping regular appointments so that we can do what is necessary to make progress, all affect the time required to complete your orthodontic treatment. Occasionally, unfavorable growth or other complications in more complex cases can prolong treatment times, but this is rare.
Usually it is safe to say, “The best cooperators get done the fastest.”
Diagnostic records
Diagnostic Records are generally where we begin treatment. These records consist of digital photographs, study models, special orthodontic radiographs and other diagnostic information. This special information is then carefully reviewed by the doctor and is the basis upon which an individual orthodontic treatment plan can be developed and reviewed with you prior to beginning treatment. It is very important to us that you completely understand what treatment is planned before we start. Other supplemental diagnostic information is often required during treatment as part of the overall plan.
Emergencies
Orthodontic emergencies are relatively infrequent today thanks to new materials and appliances that are designed to be more comfortable than those in the past. We are available to handle any problems which you may be experiencing with your orthodontic appliances. Please call us if you believe something is broken or if you have questions regarding your braces.
Malocclusion
Malocclusion is defined as poor positioning of the teeth.
Types of Malocclusion
 Class I A Malocclusion where the bite is OK (the top teeth line up with the bottom teeth) but the teeth are crooked, crowded or turned. |
 Class II A Malocclusion where the upper teeth stick out past the lower teeth. |
 Class III A Malocclusion where the lower teeth stick out past the upper teeth. This is also called an "underbite". |
Occlusion
The alignment and spacing of your upper jaw and lower teeth when you bite down.
 Openbite Anterior opening between upper and lower teeth. |
 Overbite Vertical overlapping of the upper teeth over the lower. |
 Overjet Horizontal projection of the upper teeth beyond the lower. |
 Crossbite When top teeth bite inside the lower teeth. It can occur with the front teeth or back teeth. |
Fixed and Removable Appliances
Braces: Metal and Ceramic
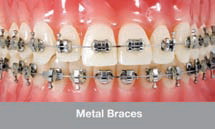 Fixed
metal braces have come a long way since the previous generation. No
longer are metal bands needed on all teeth to connect the fictional
until (bracket) to the tooth. Today we are able to bond the bracket
directly to the tooth requiring only a relatively small amount of tooth
surface to be covered. A bonding bracket is secured to the tooth surface
with dental bonding adhesive similar to that which is used for tooth
colored fillings. The area under the bracket is sealed and protected
from the outside. This means that plaque and food cannot become trapped
under the bracket. It is still important however, to brush very
carefully around the brackets since these areas are prone to being
damaged by plaque.
Fixed
metal braces have come a long way since the previous generation. No
longer are metal bands needed on all teeth to connect the fictional
until (bracket) to the tooth. Today we are able to bond the bracket
directly to the tooth requiring only a relatively small amount of tooth
surface to be covered. A bonding bracket is secured to the tooth surface
with dental bonding adhesive similar to that which is used for tooth
colored fillings. The area under the bracket is sealed and protected
from the outside. This means that plaque and food cannot become trapped
under the bracket. It is still important however, to brush very
carefully around the brackets since these areas are prone to being
damaged by plaque.
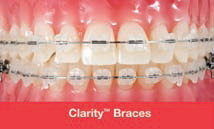 Ceramic
braces are attached the same way and perform the same functions as metal
braces. Today's ceramic (porcelain) brackets do not stain and remain the
same color throughout treatment. Ceramic braces are usually recommended
for older teens and adults for cosmetic reasons and work every bit as
well as metal braces for moving teeth.
Ceramic
braces are attached the same way and perform the same functions as metal
braces. Today's ceramic (porcelain) brackets do not stain and remain the
same color throughout treatment. Ceramic braces are usually recommended
for older teens and adults for cosmetic reasons and work every bit as
well as metal braces for moving teeth.
Most patients who wear ceramic braces are pleased to report that only their close friends and relatives can tell that they are wearing braces.
Treatment with clear aligners (Invisalign)
Treatment with clear aligners is now possible and we are very pleased offer this service. They are only one of many appliance types and systems within our orthodontic specialty. We have treated hundreds of cases with Invisalign with excellent results. However, these appliances are not suitable to treat all forms of malocclusion and dentofacial deformities. Fixed metal of ceramic braces may be a more appropriate treatment for correction of a malocclusion. As an orthodontic practice we are pleased to fully evaluate your needs and to recommend the best treatment option.

Hawley Retainers
 This
universally used retainer has many applications; to move teeth,
close spaces, maintain alignment during or after treatment.
This
universally used retainer has many applications; to move teeth,
close spaces, maintain alignment during or after treatment.
Retainers can be utilized as active appliances to move teeth and in the case of younger patients (Phase One treatment), as a growth modification device. Removable appliances have a significant role in orthodontic treatment options and will be commended as an option if appropriate for you or your child.
Retainers are also vital appliances used upon completion of the active phase of orthodontic treatment when the braces are removed.
To retain means to hold. Teeth must be retained or held in their new positions while the tissues, meaning the bone, elastic membranes around the roots, the gums, tongue and lips have adapted themselves to the new tooth positions. Teeth can move if they are not retained. It is extremely important to wear your retainers as directed!
Lower Lingual Arch (LLA)
 A
lower lingual arch is a space maintainer for the lower teeth. It
maintains
A
lower lingual arch is a space maintainer for the lower teeth. It
maintains
the molars where they are, it does not move them. This is fabricated by
placing
bands on the molars and connecting them to a wire that fits up against
the
inside of the lower teeth. It keeps the molars from migrating forward
and
prevents them from blocking off the space of teeth that develop later.
This is
used when you have the early loss of baby teeth or when you have lower
teeth
that are slightly crowded in a growing child and you do not want to
remove any
permanent teeth to correct the crowding.
Palatal Expander
 An
appliance which is placed in the roof of the mouth to widen the upper
An
appliance which is placed in the roof of the mouth to widen the upper
dental arch. The maxilla, or upper dental arch, is joined in the center
by a
joint, which allows it to be painlessly separated and spread.
Temporarily you
may see a space develop between the upper two front teeth. This will
slowly go
away in a few days. Once this has occurred, the two halves knit back
together
and new bone fills in the space.
Bi Helix
 An appliance used to expand the lower arch without interfering with
tongue posture or movement.
An appliance used to expand the lower arch without interfering with
tongue posture or movement.
 Quad
Helix
Quad
Helix
This appliance provides continual, gradual pressure in as many as four directions, to move molars, expand or contract arches or assist in eliminating finger or thumb habits.
Nance
 This appliance maintains the position of the maxillary molars without using
any other teeth. The plastic button on the palate provides
stability.
This appliance maintains the position of the maxillary molars without using
any other teeth. The plastic button on the palate provides
stability.
Early Orthodontics
The American Association for Orthodontists recommends that every child have an orthodontic evaluation by the age of 7. Early detection and treatment gives your child the edge: a much better chance for natural and normal development. By working with the natural growth instead of against it, we can prevent problems from becoming worse, and give your child a lifetime of healthy smiles!
Early treatment should be initiated for:
- Habits such as tongue thrusting and thumb sucking
- A constricted airway due to swollen adenoids or tonsils
- Mouth breathing or snoring problems
- A bad bite
- Bone problems (i.e. narrow or underdeveloped jaws)
- Space maintenance (for missing teeth)
Phase One
Functional (Growth) Appliances and/or Limited Braces – Ages 5-12
In the first phase, the doctor is interested in the position and symmetry of the jaws, future growth, spacing of the teeth, breathing and other oral habits which may, over a period of time, result in abnormal dentofacial development.
Treatment initiated in this phase of development is often very successful and sometimes, though not always, can eliminate the need for future orthodontic treatment.
Phase Two
Braces – Ages 12 to 14
In the second phase, the doctor will be looking at how your child’s teeth and jaws fit, and more specifically work, together. Your child’s teeth will be straightened and their occlusion (bite) is properly aligned. Attention will be given to the jaw joint, (TMJ), the facial profile and periodontal (gum) tissues. By undergoing the first phase, we can usually reduce the amount of time needed for braces.
Facts: Early Treatment Is Important to Consider!
Facial Development
– Seventy-five percent of 12-year-olds need orthodontic treatment. Yet 90% of a child’s face has already developed! By guiding facial and dental development earlier, through the use of functional appliances, problems can be improved before the adult teeth are present!Cooperation – Younger children between the ages of 8 and 11 are often much more cooperative than children of ages 12 to 14.
Shorter Treatment Time – Another advantage of early Phase One treatment is that children will need to wear fixed braces on their adult teeth for less time.
To Correct Underdeveloped or Overdeveloped Jaws – Almost 55% of children who need orthodontic treatment due to a bad bite have underdeveloped or overdeveloped upper or lower jaws. Functional appliances and/or limited braces can reposition the jaws, improving the child’s profile and improving the bite problem.